







آینده روان درمانی ممکن است به چه چیزی شباهت داشته باشد؟ ماهیت بی ثبات و ناپایدار این رشته نیاز مبرمی را به مشخص کردن گرایش هایی ایجاد کرده است که بر کاربست بالینی، برنامه های پژوهشی، آموزش تحصیلات عالی و سیاست گذاری تاثیر خواهند گذاشت. همگی دوست داریم وضعیت روان درمانی را در سال 2022 پیش بینی کنیم.
همانطور که ما از عصر صنعتی به عصر اطلاعات انتقال پیدا کردیم، الزامی است که از چگونگی تغییرات که بر روان درمانی، روانشناسان و بیماران اثر می گذارد، آگاه باشیم. 36 کارشناس در نظرسنجی اولیه انواع تغییرات در روان درمانی را، مانند تغییر در جهت گیری نظری از روانکاوی به شناختی-رفتاری و جایگزینی درمان طولانی مدت با درمان کوتاه مدت را پیش بینی کردند. پیش بینی های خوش بینانه و درست آنها شامل افزایش درمانگران زنان و اقلیت های قومی و همچنین تسریع بخشیدن به خدمات دادن به جمعیت محروم، اما آنها پیش بینی اشتباه تاسیس بیمه سلامت ملی هم داشتند. 75 کارشناس در دومین نظرسنجی دِلفی ما،10 سال بعد، اظهار کردند که گروه های همیاری و مددکاران اجتماعی افزایش پیدا می کنند که این باعث کاهش روان درمانی ارائه شده روانپزشکان می شود. در سال 2001، یک هیئت 62 نفره پیش بینی کردند که رهنمودهای درمانی، طب رفتاری و دارودرمانی بطور پیوسته گسترش خواهد یافت. این مطالعات، باوجود اشتباهاتی در پیش بینی، در برجسته کردن نیروهای اصلی در شکل دهی چهره روان درمانی مفید بوده اند.
ما از روش پیش بینی به نام نظرسنجی دِلفی استفاده کردیم (شروع آن به سال 1980 بر می گردد) تا آینده روان درمانی را برای 10 سال بعد پیش بینی کنیم. نظرسنجی دِلفی، ارتباط گروهی را سروسامان می دهد تا گروهی از افراد امکان یابند به مسئله پیچیده ای بپردازند. هیات متخصصان به سوال های یکسانی حداقل دوبار جواب می دهند. در مرحله اول، این متخصصان به صورت گمنام به سوال هایی بدون بازخورد جواب می دهند. در مراحل بعدی، اسامی و دیدگاه های کل اعضای هیات به این متخصصان ارایه شده و به آنها فرصت تجدید نظر در پیش بینی های خود با توجه به قضاوت گروه داده می شود.
نظرسنجی دِلفی از دیدگاه های متعدد و تعاملی متخصصان بهره مند می شوند. امتیازات خاص روش دِلفی عبارتند از (1) همواره نزدیکترین پاسخ را به سوال های بسیار دشوار در مقایسه با سایر فنون پیش آگهی فراهم می آورد؛ (2) پاسخ های بدست آمده از مرحله دوم معمولا کمتر متغیر هستند و از این رو از پاسخ های مرحله اول ابهام کمتری دارند؛ و (3) معلوم شده که اتفاق نظر گروهی از عقیده فردی متخصص دقیق تر است.
در جدیدترین نظرسنجی دِلفی که در سال 2013 انجام شد تا آینده روان درمانگری را برای دهه بعد پیش بینی کند. اعضای هیئت کارشناسان از سه نمونه گردهم آمده بودند: 34 نفر از شرکت کنندگان حاضر از مطالعه قبلی دِلفی (2001)، 54 شرکت کننده برای تاریخچه روان درمانی و 28 ویراستار از نشریات پیشتاز سلامت روان بودند.
شرکت کنندگان ابتدا پیش بینی کردند تا چه اندازه ای گرایش های نظری مختلف ظرف 10 سال بعد به کار گرفته خواهند شد. ارزیابی ها براساس مقیاس 7 امتیازی صورت گرفتند که 1=کاهش زیاد، 4=ثابت می ماند و 7=افزایش زیاد بودند. جدول زیر میانگین و رتبه 31 گرایش نظری را به ترتیب نشان می دهد.
| مرتبه | گرایش | میانگین |
| 1 | درمان های ذهن آگاهی | 55/5 |
| 2 | درمان شناختی-رفتاری | 48/5 |
| 3 | درمان یکپارچگی نظری | 23/5 |
| 4 | درمان های چندفرهنگی | 2/5 |
| 5 | درمان مصاحبه انگیزشی | 15/5 |
| 6 | رفتاردرمانی دیالکتیکی | 13/5 |
| 7 | درمان التقاطی | 85/4 |
| 8 | درمان های مواجه سازی | 85/4 |
| 9 | درمان میان فردی | 81/4 |
| 10 | درمان شناختی | 79/4 |
| 11 | درمان مبتنی بر پذیرش و تعهد | 7/4 |
| 12 | درمان سیستمی و خانواده | 53/4 |
| 13 | درمان مبتنی بر دلبستگی | 51/4 |
| 14 | رفتار درمانی | 43/4 |
| 15 | رابطه درمانی | 18/4 |
| 16 | درمان تجربی | 02/4 |
| 17 | روایت(قصه) درمانی | 94/3 |
| 18 | درمان راه حل مدار | 9/3 |
| 19 | درمان روانپویشی | 79/3 |
| 20 | درمان فردمدار | 59/3 |
| 21 | درمان انسان گرا | 55/3 |
| 22 | درمان فمینیستی | 44/3 |
| 23 | درمان حساس نسبت به مردان | 4/3 |
| 24 | درمان وجودی | 3 |
| 25 | درمان حساسیت زدایی با حرکت چشم و پردازش مجدد | 71/2 |
| 26 | درمان گشتالتی | 65/2 |
| 27 | واقعیت درمانی | 48/2 |
| 28 | درمان روانکاوی(کلاسیک) | 15/2 |
| 29 | درمان یونگی | 1/2 |
| 30 | درمان آدلری | 84/1 |
| 31 | درمان فرانظری | 81/1 |
به طوری که در این جدول دیده می شود، درمان های ذهن آگاهی، شناختی-رفتاری، یکپارچه، چندفرهنگی، مصاحبه انگیزشی، رفتاردرمانی دیالکتیکی، التقاطی و مواجهه سازی در دهه بعد بالاترین افزایش و در مقابل، درمان های فرانظری، آدلری، یونگی و روانکاوی بیشترین کاهش را خواهد داشت.
اعضای هیات همچنین افزایش و کاهش نسبی 45 مداخله درمانی را پیش بینی کردند. پیش بینی شد که از 45 مداخله، 19 مداخله در دهه بعدی افزایش یابند. پیش بینی شد که روش هایی که با تکنولوژی کامپیوتر مشخص می شوند (واقعیت مجازی، درمان های کامپیوتری)، تغییر خود درمانجو (تغییر خود، منابع خودیاری، روش های کنترل خود) و رهنمودهای درمانگر یا روش های ساختن مهارت (تکالیف خانگی، پیشگیری از بازگشت، فنون حل مسئله و بازسازی شناختی) از همه بیشتر افزایش می یابند. از سوی دیگر، تداعی آزاد، تمرین های رویارویی، غرقه سازی هیجانی و تجسمی و تعبیر رویا از همه بیشتر کاهش خواهند یافت.
در آخر متخصصان، محبوبیت آینده 9 نوع (قالب بندی) را نیز پیش بینی کرده اند. آنها درمان کوتاه مدت، مراقبت های روانی در خانه، درمان خیلی کوتاه مدت، گروه های روانی آموزشی برای اختلالات خاص، مداخله در بحران و مداخلات در سطح جمعیت رو به افزایش می دانند و انتظار می رود 4 قالب بندی در آینده تغییر نکنند: زوج درمانی یا درمان زناشویی، گروه درمانی، درمان فردی و خانواده درمانی مشترک.
.
.
منبع:
Norcross. J,. Pfund. A,. Prochaska. J. Psychotherapy in 2022: A Delphi Poll on Its Future. (2013). Professional Psychology: Research and Practice. Vol. 44, No. 5, 363–370.
.
.
Psychotherapy in 2022: A Delphi Poll on Its Future
What might psychotherapy look like in the next decade? Where are the growth opportunities and the probable dinosaurs for psychologists? How can seasoned practitioners, early career psychologists, and graduate students best prepare themselves for that evolving future? What will prove hot—and not—in 2022?
As we transition from the industrial era to an information era, it is imperative that we remain knowledgeable of how changes will impact psychotherapy, psychologists, and our patients (Lesse, 1987). The existence of time and the laws of physics make the future inevitable, and it will prove advantageous to reflect on and plan for where psychotherapy is heading. What does the future hold in terms of theories, methods, providers, formats, and developments? All of us—practitioners, educators, researchers, policymakers, and students—have a profound stake in the future of the discipline.
Every 10 years, starting in 1980 (Norcross, Alford, & DeMichele, 1992; Norcross, Hedges, & Prochaska, 2002; Prochaska & Norcross, 1982), we have conducted a Delphi poll on the future of psychotherapy. The 36 experts in the initial poll anticipated a variety of changes in psychotherapy, such as the shift in theoretical orientation from psychoanalytic to cognitive– behavioral and the replacement of long-term therapy with briefer therapy. Their optimistic and correct forecasts included an increase in female and ethnic minority therapists as well as accelerated services to underserved populations, but they erroneously foresaw the establishment of national health insurance. The 75 experts in our second Delphi poll, 10 years later, opined that self-help groups and social workers would proliferate and that the proportion of psychotherapy provided by psychiatrists would diminish. In 2001, a panel of 62 prognosticated that practice guidelines, behavioral medicine, and pharmacotherapy would steadily expand.
These studies, despite the occasional miss in judgment, have highlighted core forces that are persistently shaping the face of psychotherapy. Following the 10-year tradition, we repeated and expanded a Delphi poll to garner an expert consensus on psychotherapy during the next decade.
The Delphi Method
Developed in the early 1950s by the Rand Corporation as a part of military research on expert opinion, the Delphi methodology structures communication so that a group can collectively grapple with a complex problem and efficiently render reasonably accurate opinions on future events or directions (Linstone & Turoff, 1975). “The Delphi approach is particularly well-suited for emerging areas of inquiry and for building consensus among a group of experts. When it is used for these purposes, few weaknesses exist” (Fish & Busby, 1996, p. 478). In fact, research demonstrates that the results of Delphi polls usually provide the most accurate answers to difficult questions compared with other prognostication techniques (Boronson, 1980; Parente & Anderson-Parente, 2011). The group Delphi consensus also consistently outperforms individual expert opinion (Ascher, 1978; Linstone & Turoff, 1975). For all these reasons, the Delphi has a lengthy tradition as a robust research method, especially in the health sciences (Donohue, Stellefson, & Tennant, 2012) and increasingly in psychology (e.g., James & Roberts, 2009; Neimeyer, Taylor, & Rozensky, 2012).
A panel of experts answers the same questions at least twice. In the first round, the experts answer the questions anonymously and without knowledge of the responses of their peers. During subsequent rounds, the experts are provided with the responses of the entire panel and are given the opportunity to revise their predictions in light of the group judgment. The accuracy of probability forecasts increases over Delphi rounds, up to the second round (Martino, 1972; Ascher, 1978), and when statistical summaries are provided to the experts (Rowe, Wright, & McColl, 2005).
We created a multipage, electronic questionnaire on Survey- Monkey based on our previous Delphi polls. Dated items were eliminated and new items were added to reflect recent developments; three-quarters of the items appeared on one or more of the previous polls. The questionnaire comprised five sections: theoretical orientations (31 items), therapeutic interventions (45 items), psychotherapists (18 items), therapy formats (11 items), and forecast scenarios (25 items).
The panel was repeatedly asked to predict the probability of each item increasing or decreasing during the next 10 years. We requested “your prediction of what will happen, as opposed to what you personally would like to happen.” In this way, we hoped to minimize wishes disguised as predictions, since many forecasts in the uncertain world of psychotherapy tend to resemble selffulfilling prophecies or magical wishes (Ekstein, 1972).
Responses on the first four sections were recorded on a 7-point, Likert-type scale where 1 _ great decrease, 2 _ moderate decrease, 3 _ slight decrease, 4 _ remain the same, 5 _ slight increase, 6 _ moderate increase, and 7 _ great increase. Responses to the final section were recorded in a similar fashion, where 1 _ very unlikely, 2 _ moderately unlikely, 3 _ slightly unlikely, 4 _ uncertain, 5 _ slightly likely, 6 _ moderately likely, and 7 _ very likely.
Our procedure followed conventional Delphi methodology. A letter containing a link to the questionnaire was emailed to the expert panel in June 2012. Their responses were pooled and analyzed. The same questionnaire was redistributed to the panelists in mid-July, along with the means and standard deviations on all items from the first round. Those data were depicted both numerically and graphically on the second round questionnaire. Individual responses were not (and could not be) identified.
The Expert Panel
Members of the expert panel came from three samples: the 34 living participants of our previous Delphi study (Norcross et al., 2002), 58 contributors to the History of Psychotherapy (Norcross, VandenBos, & Freedheim, 2010), and 28 editors of leading mental health journals. Seventy-three (61%) of these 120 possible panelists returned the first round of the questionnaire, but three were not usable, leaving 70 participants. Sixty-two of the 70 (89%) completed the second round of the poll.
The panel consisted of distinguished and experienced mental health professionals. All 70 panelists held a doctorate (66 PhDs, 2 EdDs, 1 MD, 1 PsyD) and related an average of 33 years (SD _ 11.56) of postdoctoral clinical experience. The panel was composed of 16 women and 51 men (three did not indicate gender). The questionnaire did not contain an item on the respondent’s race or ethnicity, which in retrospect proved an unfortunate oversight.
On average, the panelists devoted 33% of their professional time to research/writing, 23% to administration, 21% to teaching, 19% to clinical work, 12% to supervision, and 17% to other activities. The most prevalent employment settings were university departments (73%), private practices (9%), and medical schools (6%). Theoretical orientation was assessed by asking the experts to select from a list of 20 possibilities, including “other.” The experts represented a diversity of self-reported theoretical orientations: integrative/eclectic (29%), cognitive– behavioral (29%), psychodynamic (10%), humanistic/experiential (9%), other (8%), systems/ family systems (4%), relational (4%), interpersonal (3%), behavior therapy (2%), and psychoanalysis (2%).
Results and Discontents
central goal of Delphi methodology is to reach a consensus among the experts. The achievement of this goal was illustrated by consistent decreases in item standard deviations from the first to the second round. This occurred for 93 of the 130 items (72%). Providing feedback to the panel of experts reduced disparity and encouraged consensus concerning future directions in psychotherapy.
At the same time, the limitations of this study and of the expert panel in particular should be borne in mind while interpreting the forecasts. First, our panel was composed of psychotherapists living and working in the United States; generalizations to other countries are unwarranted. Second, the relative paucity of women on the expert panel (24%) does not reflect the field as it is developing. However, statistical analyses revealed practically no differences between the predications of men and women. Third, the panel was composed primarily of those working in university departments and medical schools; it is possible that the predictions were slanted toward teaching, training, and gatekeeping functions (e.g., journal editing) as opposed to practice considerations. Our analyses did not reveal any pattern of consistent differences due to employment setting, however. Fourth, our experts’ predictions do not reflect absolute changes but rather relative increases and decreases. A theoretical orientation or a clinical method could increase substantially in the next decade but still not be a common event. Fifth, our sample included only one psychiatrist; these are forecasts by and for psychologists. And sixth, readers should be mindful of the pitfalls of prediction and probability. Many predictions fail because of a poor understanding of probability and uncertainty; overconfidence is often the reason for inaccuracy (Silver, 2012).
The following tables present the item means and standard deviations from both data waves, but the items are rank-ordered in terms of the results of the second wave. Lines in the tables divide the items into three rationally created categories: those items the experts expect to increase (item mean of 4.5 and greater), those items predicted to remain about the same (mean ranging from 3.5 to 4.49), and those predicted to decrease (mean of 3.49 and less) in the next decade.
Theoretical Orientations
Our experts rated the extent to which a variety of psychotherapy systems will be used over the next decade. As presented in Figure 1, 13 systems were predicted to increase, 8 to stay about the same, and 10 to decrease. Those orientations expected to increase the most were mindfulness, cognitive– behavioral, integrative, multicultural, motivational interviewing, dialectical behavior, eclectic, and exposure therapies. By contrast, transactional analysis, Adlerian therapy, Jungian therapy, and classical psychoanalysis were expected to decrease the most.
We repeatedly emphasized that panelists should predict what would happen rather than what they would like to happen. But, in addition to being experts, our observers might be prone to present their own preferred theories in a more favorable light. To investigate the possibility of a rating bias due to theoretical orientation, we compared the average predictions of endorsers of three superordinate orientations: integrative/eclectic (n _ 20), cognitive– behavioral (n _ 18), and insight-oriented (psychodynamic, psychoanalytic, and humanistic; n _ 11). Panelists who identified themselves as insight-oriented rated the future of psychodynamic therapy significantly more favorably (M of 4.60 vs. 2.83 and 4.29, p _ .05) than did the cognitive–behaviorists and integrative/eclectics. Integrative/eclectic therapists, in turn, rated the future of integrative therapy significantly higher (M of 5.69 vs. 4.72, p _ .05) than did the insight-oriented. However, no differential ratings were made on the future of cognitive–behavioral therapy. When we compared ratings on the 31 theoretical orientations, we determined that only six were statistically different due to the experts’ orientations. Thus, there was robust convergence in predictions but modest allegiance bias with regard to the experts’ favored theories.
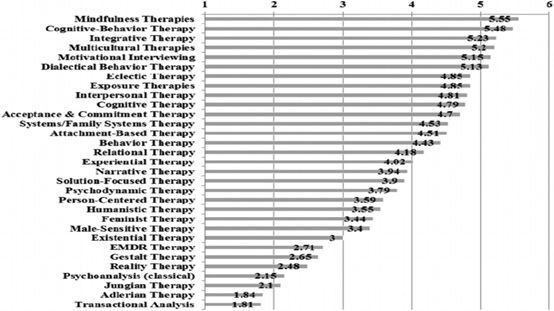
Figure 1. Predicted changes in theoretical orientations in rank order. 1 _ great decrease, 4 _ remain the same,
7 _ great increase. EMDR _ eye movement desensitization and reprocessing.
Therapeutic Interventions
19 of the 45 listed interventions were predicted to increase in the next decade. Computer technology (online self-help, smartphone applications, virtual reality, social networking interventions), client self-change (self-help resources, bibliotherapy, self-help techniques, self-control proce- dures), and skill building methods (relapse prevention, homework assignments, problem-solving techniques, cognitive restructuring) were forecast to increase the most. Accompanying these high-tech, directive methods were the high-touch, interpersonal processes of fostering the therapeutic alliance, providing interpersonal support, and expressing warmth and caring, all in the top 15. Panelists forecasted that aversive conditioning, free association, encounter exercises, and dream interpretation would diminish the most.
Therapy Formats
Our experts foresee short-term therapy, psychological care in medical homes, very short-term therapy, psychoeducational groups, crisis intervention, and population-level interventions as increasing in the next 10 years. Couple/marital, group, individual, and conjoint family therapies were expected to experience essentially no change in the future. As in the last Delphi poll, our panel members forecasted that only one therapy format would decline: long-term therapy.
Reference
Norcross. J,. Pfund. A,. Prochaska. J. Psychotherapy in 2022: A Delphi Poll on Its Future. (2013). Professional Psychology: Research and Practice. Vol. 44, No. 5, 363–370.
.
.
روان درمانی در سال 2022 : نظرسنجی دِلفی
جان نورکراس – روری پفوند – جیمز پروچسکا
Psychotherapy in 2022: A Delphi Poll on Its Future
روان درمانی در سال 2022 : نظرسنجی دلفی درباره آینده روان درمانی
مترجم: حسین فرخی (دانشجوی کارشناسی ارشد روانشناسی بالینی دانشگاه علامه طباطبائی)
.
.